Cardiac screening before symptoms appear: why it matters and how it works
Most heart conditions do not announce themselves. They develop silently over months and years, causing damage long before any noticeable symptoms emerge. Cardiac screening before symptoms appear is the single most effective clinical strategy for catching these conditions early – when they are still manageable, treatable, and even reversible.
What is presymptomatic cardiac screening?
Presymptomatic cardiac screening refers to the process of evaluating the heart’s health in individuals who have no current cardiac complaints no chest pain, no breathlessness, no palpitations. The goal is not to diagnose an existing illness but to identify subclinical abnormalities, elevated risk markers, and early structural or functional changes before they cause clinical symptoms or irreversible damage.
Unlike reactive medicine which responds to what has already gone wrong presymptomatic screening is a form of proactive cardiovascular care. It operates on a foundational principle: the earlier a problem is identified, the wider the window of intervention available, and the better the long-term outcome for the patient.
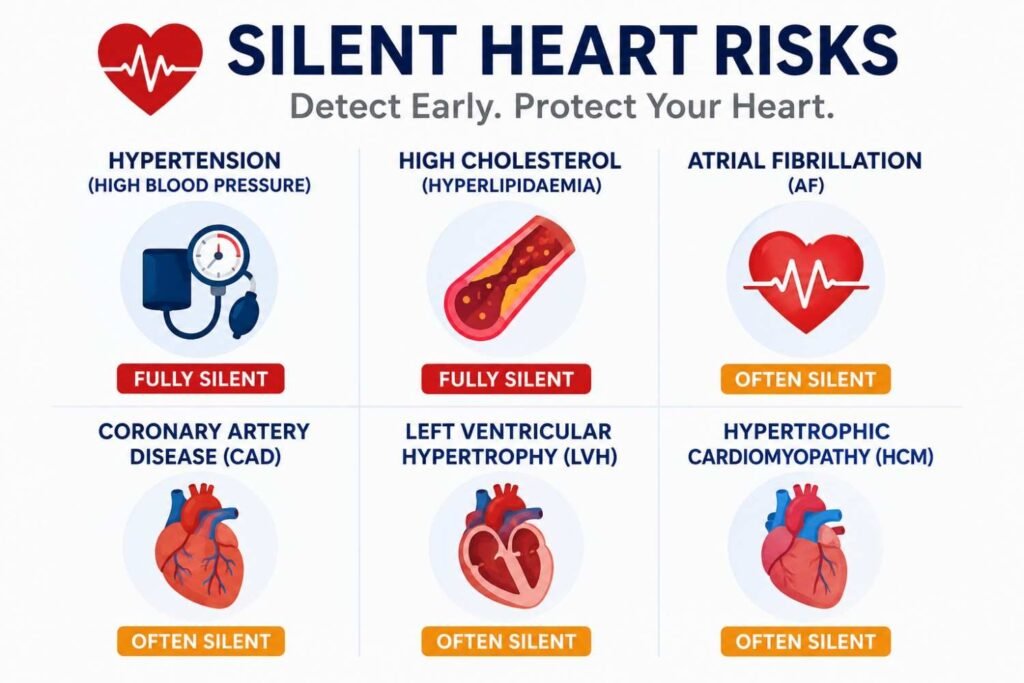
Heart conditions that develop without symptoms
Several of the most clinically significant cardiovascular conditions are characterised by an extended presymptomatic phase a period during which the disease is actively progressing but the patient experiences nothing out of the ordinary. This is what makes them particularly dangerous, and what makes early screening so essential.
Why waiting for symptoms is dangerous?
The instinct to act only when something feels wrong is understandable, but in the context of heart disease it is medically counterproductive. By the time most cardiac conditions produce noticeable symptoms, the underlying disease process has typically been underway for years and may have already caused structural damage that cannot be fully reversed.
What happens when you wait?
- Silent damage accumulates over years
- Arterial plaques grow and harden
- Blood pressure stays uncontrolled
- Heart muscle adapts and remodels
- Treatment options become more limited
- Risk of acute cardiac event increases
What early screening enables
- Identification of risk before damage occurs
- Medication initiated at the right time
- Lifestyle changes while still impactful
- Structural problems caught while mild
- Broader, less invasive treatment choices
- Significantly better long-term outcomes
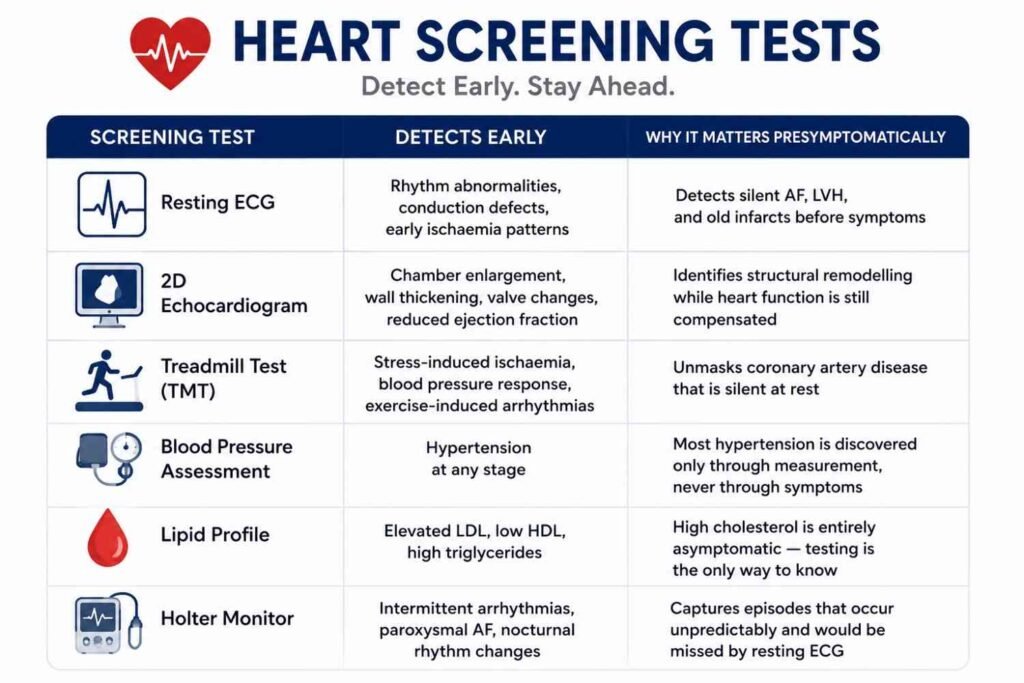
How screening detects problems before symptoms
Cardiac screening tests are designed to detect physiological and structural changes that precede symptomatic disease. Each test examines a different clinical dimension and is capable of identifying abnormalities at a stage when the patient still feels well.
Common myths vs facts about presymptomatic screening
Several widely held beliefs discourage people from seeking cardiac screening before they feel unwell. Here is what the evidence actually shows.
Myth
If I had a heart problem, I would feel it
Fact
Most cardiac conditions — hypertension, high cholesterol, AF, early CAD – produce no symptoms until advanced. Feeling well is not clinical evidence of a healthy heart.
Myth
Heart disease only affects older people
Fact
Atherosclerosis begins in the twenties and thirties. Risk factors accumulate for decades before causing clinical events. Early screening is precisely what prevents premature heart disease.
Myth
Exercise means my heart must be fine
Fact
Physical fitness reduces many risk factors but does not eliminate cardiac conditions. Hypertrophic cardiomyopathy, AF, and structural valve disease can be present in highly active individuals with no apparent limitation.
Cardiac screening vs cardiac diagnosis
These two terms are often used interchangeably but they represent fundamentally different clinical processes with different goals and patient populations.
Both processes use many of the same tests – ECG, echocardiogram, TMT – but the clinical context, urgency, and implications differ significantly. Screening at the presymptomatic stage is always preferable because it operates upstream of disease, before damage has accumulated.
Cardiac screening
- Performed on asymptomatic individuals
- Goal is to detect risk or early disease
- Proactive and preventive in intent
- Scheduled periodically based on risk
- May or may not reveal an abnormality
- Prevents disease progression
Cardiac diagnosis
- Performed in response to symptoms
- Goal is to identify the cause of complaints
- Reactive and investigative in intent
- Triggered by chest pain, breathlessness, etc.
- Expected to find a clinical explanation
- Manages existing disease
Lifestyle changes that work alongside screening
Presymptomatic cardiac screening is most powerful when combined with consistent heart-healthy habits. Screening identifies what is happening inside the cardiovascular system; lifestyle choices determine the direction it is heading.
- A diet low in saturated fat, salt, and refined carbohydrates reduces cholesterol and blood pressure the two most common silent risk factors detected on screening
- Regular moderate aerobic exercise (at least 150 minutes per week) improves cardiac efficiency, lowers resting heart rate, and reduces arterial stiffness
- Maintaining a healthy body weight reduces the cardiac workload and lowers the risk of metabolic syndrome, diabetes, and hypertension
- Smoking cessation at any age produces measurable cardiovascular benefits within months and significantly lowers long-term cardiac risk
Conclusion
Cardiac screening before symptoms appear is one of the most important investments a person can make in their long-term health. The heart is uniquely vulnerable to silent disease conditions that cause no pain, no discomfort, and no warning until they have reached a critical or irreversible stage. Presymptomatic screening changes this dynamic entirely by providing a clinical window into cardiovascular health at a stage when intervention is most effective. Whether you are in your thirties and building a health baseline, in your forties navigating rising risk factors, or at any age managing conditions like hypertension or diabetes, proactive cardiac evaluation is the most reliable path to a longer, healthier life. Do not wait for symptoms to appear. Schedule a cardiac screening today because the best time to protect your heart is before it asks for help.
For evidence-based guidelines on cardiovascular disease prevention and presymptomatic risk reduction, visit the American Heart Association — a globally recognised authority on heart health for patients and healthcare professionals.